Int J Drug Res Clin. 2023;1:e4.
doi: 10.34172/ijdrc.2023.e4
Original Article
Evaluation of Pain Relief in Trauma Patients and Patients’ Satisfaction
Paria Habibollahi 1  , Samad Shams Vahdati 2, Neda Karzad 2, Samad Gholzari 3, 4, Masoumeh Poureskandari 2, *
, Samad Shams Vahdati 2, Neda Karzad 2, Samad Gholzari 3, 4, Masoumeh Poureskandari 2, *
Author information:
1Toxicology and Pharmacology Department, Pharmacy Faculty, Tabriz University of Medical Sciences, Tabriz, Iran
2Emergency and Trauma Care Research Center, Tabriz University of Medical Sciences, Tabriz, Iran
3Department of Anesthesiology and Intensive Care Medicine, Dortmund General Hospital, Dortmund, Germany
4Department of Health, Witten-Herdecke University, Witten, Germany
Abstract
Background:
Trauma patients are the most frequent patients admitted to the emergency department. Pain management is one of the most critical goals in these patients. This study aimed to assess the use of analgesics effect to control pain in trauma patients.
Methods:
All trauma patients (72 men and 19 women) aged 18 to 80 years who were referred to the emergency department between April and August 2020 were studied. Following the primary survey, the patient’s pain was assessed using the visual analog scale, and an analgesic medication was administered based on an emergency medicine specialist’s choice. The patient’s pain level and satisfaction with pain management were assessed after half an hour. The analgesic drug was selected at the discretion of the relevant specialist, and no particular analgesic drug was considered.
Results:
The average pain level in the pre-treatment group was 55 mm. After obtaining analgesia, this number was reduced to 26 mm. The type of medicine prescribed, the patient’s age and sex, the patient’s satisfaction with pain management, and the type of trauma all influenced the patient’s response to pain management. Moreover, opioid pain relief was preferred by patients over non-steroidal anti-inflammatory drugs (NSAIDs) or paracetamol.
Conclusion:
In trauma patients, analgesics have a major effect on pain management, and patient satisfaction rises as analgesia is used effectively. In most cases, NSAIDs are the medication of choice; however, opioids are prescribed for the elderly and patients with serious and intolerable pain.
Keywords: Analgesia, Trauma, Satisfaction
Introduction
Pain is an uncomfortable physical and emotional feeling caused by different forms of injury.1 Most pains disappear after the unpleasant stimulation is withdrawn, and the body recovers, but sometimes the pain continues despite the removal of stimuli and the improvement of body’s appearance. In addition, sometimes, the pain exacerbates due to the absence of observable conditions of the original injury.2
In medical terminology, a traumatic injury is any form of injury, stroke, laceration, shock, or accident to the human body that occurs from the outside and is not induced by an internal cause of disease in the body. Trauma is the sixth most common cause of death according to statistics.3 It can be categorized depending on the site of the injury (e.g., head trauma, abdominal trauma, and the like) or the characteristics of the trauma-causing factors (penetrating or blunt trauma and thermal or compressive trauma).3-7 Controlling pain for patient satisfaction is one of the most important goals in managing trauma patients. This study aimed to find out how analgesic medications affected pain management in trauma patients and how to use these drugs effectively in the emergency department.
Methods
In this descriptive-analytical study, patients who were admitted to the emergency department of trauma center of North-west of Iran due to trauma were assessed for pain and their satisfaction with pain management from April to August 2020. A total of 91 patients were included in the survey. The exclusion criteria were patients under the age of 18, patients with Glasgow Coma Scale 14 or less, and patients with a history of opioids or painkiller addiction. Furthermore, patients’ demographic details such as age, sex, and drug history were reported on a checklist during a face-to-face interview in the hospital emergency room. Pre-treatment pain severity, post-analgesic pain severity, and patient satisfaction with pain management were among the analyzed variables.
Following the primary survey, the patient’s pain was determined using visual analogue pain scale parameters. Then, the analgesic medication was injected based on the specialist’s choice. For half an hour, the patient was assessed and asked about the level of pain and satisfaction of pain management. No specific analgesic drug was considered, and drugs were used based on physician’s preference.
Statistical Analysis
Statistical analysis was performed using the SPSS statistical software (SPSS 17.0 for Windows; SPSS Inc., Chicago, IL, USA). P value under 0.05 was considered statistically significant. Quantitative and qualitative variables were presented as frequency and percentage, respectively. Further, Pearson correlation and logistic regression methods were used to investigate the relationship between the collected data. Then, paired t test was used to compare the severity of pain before and after analgesic administration.
Results
A total of 91 patients aged 18 to 80 years were studied (P value = 0.001), with 72 (79.1%) males and 19 (20.9%) females (Table 1).
Table 1.
Demography of Patients and Trauma
|
Variable
|
|
| Gender, No. (%) |
|
| Male |
72 (79.1) |
| Female |
19 (20.9) |
| Age, No. (%) |
|
| 18–39 |
49 (58.2) |
| 40–59 |
25 (27.5) |
| 60–80 |
13 (14.3) |
| Emergency classification, No. (%) |
|
| Car crash with car |
9 (9.9) |
| Car crash with bike/motorcycle |
4 (4.4) |
| Car to pedestrian accident |
20 (22) |
| Car overturning |
14 (15.4) |
| Bike/motorcycle overturning |
15 (16.5) |
| Fall down |
24 (26.4) |
| Other |
5 (5.5) |
| Analgesics used (%) |
|
| NSAIDs |
46% |
| Paracetamol |
29% |
| Opioid |
25% |
| History of drug use, No. (%) |
|
| Negative |
82 (90.1%) |
| Positive |
9 (9.9%) |
The results indicated that falling and car to pedestrian accident were the most common causes of trauma. In most patients, NSAIDs were used to control pain (Table 1). At baseline, the average pain of patients was 55 mm, which decreased to 26 mm after the administration of analgesic (Figures 1 and 2).
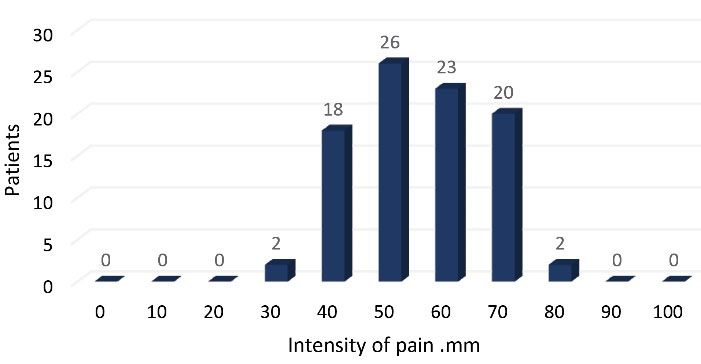
Figure 1.
The Number of Patients Categorized Based on Severity of Pain before Treatment
.
The Number of Patients Categorized Based on Severity of Pain before Treatment
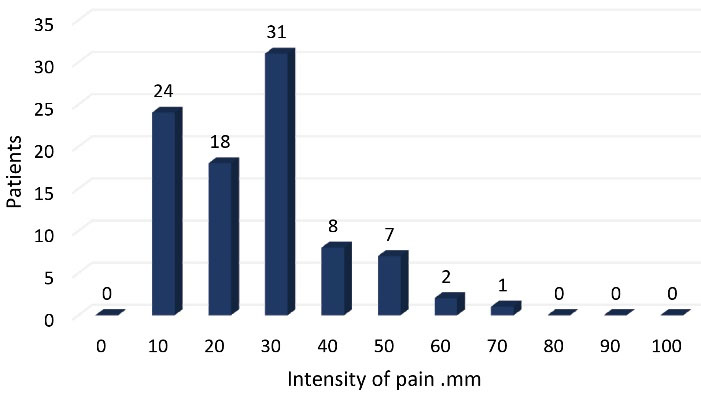
Figure 2.
The Number of Patients Categorized based on the Severity of Pain after Treatment
.
The Number of Patients Categorized based on the Severity of Pain after Treatment
The type of drug, the patient’s age and sex, the type of trauma, and the patient’s satisfaction with pain control all influenced how well analgesic therapy worked. The age of the patients had an inverse relation with the type of pain treatment. Opioid preference was higher in elderly patients (P = 0.001, Correlation coefficient = -0.452). The type of drug used to manage the patient’s pain was inversely related to the severity of the pain before treatment; in situations where the pain was more serious, opioids were more likely to be chosen (P = 0.006, Correlation coefficient = -0.356). Women had more pre-treatment pain tolerance and pain management performance than men (P = 0.006, Correlation coefficient = 0.282). The type of medications had an inverse correlation with patient satisfaction. As compared to paracetamol or NSAIDs, patients were more satisfied with opioid administration. More than 50% of patients were satisfied with pain control (Figure 3).
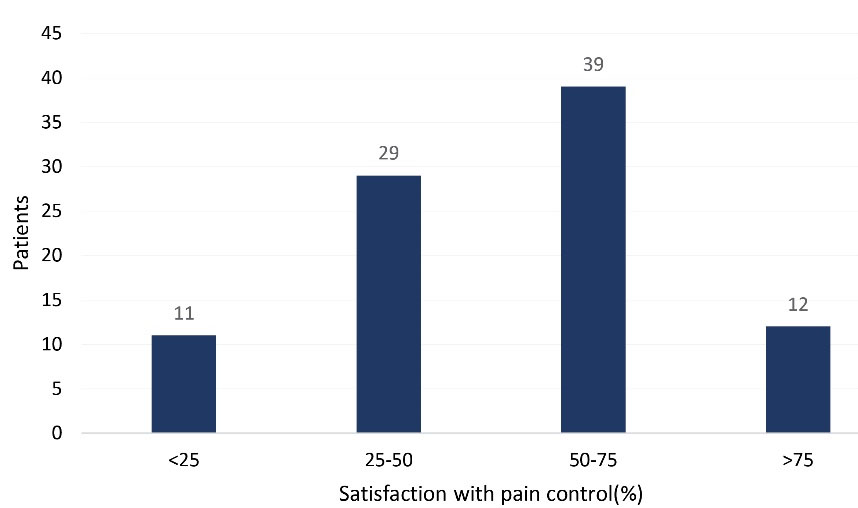
Figure 3.
Patients’ Satisfaction with Pain Control
.
Patients’ Satisfaction with Pain Control
Discussion
According to this study, most trauma patients were young working-age men. Trauma patients were in intense pain and needed analgesics immediately. Trauma patients have a high response rate to analgesic therapy. Women experienced more discomfort and had a lower pain tolerance than men. Patients who were satisfied with their special care most likely return to the emergency department if their pain did not go away.8,9 However, a significant number of patients (between 20% and 50%) were dissatisfied with the pain management care provided by the emergency department.10
Merskey defined pain as “a sensitive and unpleasant emotional experience with actual or potential tissue damage.” Trauma pain is one of the main causes of pain.11 According to the Royal College of Emergency Physicians, patients with severe pain can receive pain relief within 20 minutes of presenting in the emergency department. However, in most trauma patients, the analgesic effect is ineffective and, almost half of the patients thought that more should be done in the emergency department to treat their pain.12 NSAIDs help reduce acute pain in combination with other agents. By inhibiting prostaglandin synthesis, they have analgesic, anti-inflammatory, and antipyretic effects.13 Paracetamol is an important analgesic that is often used as a complement to opioid analgesia. It also has the antipyretic effect.13 It is quickly consumed after oral administration. It has few side effects, but patients with active liver disease should be used with caution.14 High potent opioids including morphine, oxycodone, and fentanyl are the most common type of pain medication used to treat mild to severe pain.13 Morphine is the most commonly used drug in the treatment of acute pain, and it is also used as the first line of treatment of pain caused by serious trauma. It is also prescribed as patient-controlled analgesia. Sedation, constipation, nausea, and vomiting are all common side effects of opioids.15
Limitation
In this study, because of the cross-sectional study, we cannot compare the analgesic or choose any specific analgesic, there, the potency of analgesics cannot be measured and only we can measure the efficacy of analgesics in controlling pain. Also, we cannot omit the effect of age and sex in the efficacy of analgesics. It seems that designing the prospective study with a specific analgesic can improve the strengths of study.
Conclusion
Proper and effective use of analgesics in trauma patients reduces patients’ pain significantly. NSAIDs are commonly used as the first line of treatment. Opioids are preferred by the elderly and patients with severe pain, because they are more accessible, have fewer side effects, and are safer.
Ethics statement
This study was approved by the regional Ethics Committee of Azad University, Tabriz branch, Tabriz, with registry no. IR.IAU.TABRIZ.REC.1399.128.
Disclosure of funding source
This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.
Conflict of interests declaration
The author(s) declared no potential conflict of interests with respect to the research, authorship, and/or publication of this article.
Acknowledgements
The authors would like to thank all of the participants in the study as well as nurses, staffs, and colleagues who cooperated in conducting this study.
References
- Turk DC, Dworkin RH. What should be the core outcomes in chronic pain clinical trials?. Arthritis Res Ther 2004; 6(4):151-4. doi: 10.1186/ar1196 [Crossref] [ Google Scholar]
- Casey KL, Melzack R. Sensory, motivational, and central control determinants of pain: a new conceptual model. In: Kenshalo DR, ed. The Skin Senses. Charles C Thomas Publisher; 1968. p. 423-39.
- Søreide K. Epidemiology of major trauma. Br J Surg 2009; 96(7):697-8. doi: 10.1002/bjs.6643 [Crossref] [ Google Scholar]
- Breivik H, Borchgrevink PC, Allen SM, Rosseland LA, Romundstad L, Hals EK. Assessment of pain. Br J Anaesth 2008; 101(1):17-24. doi: 10.1093/bja/aen103 [Crossref] [ Google Scholar]
- Campbell JN. APS 1995 Presidential address. Pain Forum 1996; 5(1):85-8. doi: 10.1016/s1082-3174(96)80076-6 [Crossref] [ Google Scholar]
- Joint Commission on Accreditation of Healthcare Organizations. Pain Standards for 2001. CAMH Refreshed Core; 2001. Available at: https://jointcommission.org. Accessed April 24, 2018.
- Joint Commission Resources. Comprehensive Accreditation Manual for Hospitals. Oak Brook, IL: Joint Commission Resources; 2017.
- The Joint Commission on Accreditation Survey. Available at: https://hcahpsonline.org. Accessed April 24, 2018.
- Available at: https://www.qualitymeasures.ahrq.gov/summaries/summary/51203.
- Yaster M, Benzon HT, Anderson TA. “Houston, we have a problem!”: the role of the anesthesiologist in the current opioid epidemic. Anesth Analg 2017; 125(5):1429-31. doi: 10.1213/ane.0000000000002395 [Crossref] [ Google Scholar]
- Merskey H. Pain terms: a list with definitions and notes on usage Recommended by the IASP Subcommittee on Taxonomy. Pain 1979; 6(3):249. [ Google Scholar]
- Todd KH, Ducharme J, Choiniere M, Crandall CS, Fosnocht DE, Homel P. Pain in the emergency department: results of the pain and emergency medicine initiative (PEMI) multicenter study. J Pain 2007; 8(6):460-6. doi: 10.1016/j.jpain.2006.12.005 [Crossref] [ Google Scholar]
- Keene DD, Rea WE, Aldington D. Acute pain management in trauma. Trauma 2011; 13(3):167-79. doi: 10.1177/1460408611400813 [Crossref] [ Google Scholar]
- Remy C, Marret E, Bonnet F. Effects of acetaminophen on morphine side-effects and consumption after major surgery: meta-analysis of randomized controlled trials. Br J Anaesth 2005; 94(4):505-13. doi: 10.1093/bja/aei085 [Crossref] [ Google Scholar]
- Hudcova J, McNicol E, Quah C, Lau J, Carr DB. Patient controlled opioid analgesia versus conventional opioid analgesia for postoperative pain. Cochrane Database Syst Rev. 2006(4):CD003348. 10.1002/14651858.CD003348.pub2.