Int J Drug Res Clin. 2:e10.
doi: 10.34172/ijdrc.e10
Original Article
Therapeutic Effects of Intralesional Injection of Vitamin D3 in Treatment of Recalcitrant Warts: An Evaluator-Blinded Clinical Trial
Afsaneh Radmehr 1  , Armaghan Ghareaghaji Zare 1 , Sina Radmehr 2 , Zahra Abdossamadi 3, *
, Armaghan Ghareaghaji Zare 1 , Sina Radmehr 2 , Zahra Abdossamadi 3, *
Author information:
1Department of Dermatology, Sina Hospital, Tabriz University of Medical Science, Tabriz, Iran
2School of Medicine, Iran University of Medical Science, Tehran, Iran
3Student Research Committee, Tabriz University of Medical Sciences, Tabriz, Iran
Abstract
Background:
Viral warts are a prevalent infection that affects people all over the world. Unfortunately, there is no proven antiviral treatment for them. Recalcitrant warts are also difficult to resolve and deciding on a strategy for their treatment is challenging. Recently immunotherapy modalities have led to desired treatment outcomes in patients. This study investigated the efficacy of vitamin D injection (as an immunotherapeutic agent) in the treatment of recalcitrant warts.
Methods:
In this clinical trial study, 40 patients were divided into two groups: the first group (intervention group) received cryotherapy with an intralesional injection of vitamin D3 (0.1 cc of vitamin D3 (300000 IU/1mL) per lesion and a maximum of 0.5 cc per session), and the second group (control group) received just cryotherapy. In each treatment session, patients were evaluated for treatment responses and any side effects. Each patient received four treatment sessions at 2-week intervals.
Results:
After 4 treatment sessions, the rate of response in the intervention group and the group that received just cryotherapy was 95.33%±5.87 and 76.67%±25.14, respectively, and this difference was significant (P<0.01). Furthermore, 57% (26 out of 45) of the lesions in the intervention group were completely resolved after 4 sessions, and the rest showed a moderate response to this treatment. Moreover, the minimum response rate was 80% in the intervention group and 30% in the control group.
Conclusion:
In recalcitrant skin warts, intralesional injection of vitamin D3 combined with cryotherapy significantly increased the treatment response and reduced the financial burden imposed on patients. The limitation of this trial was the small sample size of patients without a follow-up plan after completing the treatment sessions.
Trial registration:
The Iranian Registry of Clinical Trials registered this study (identifier: IRCT20200513047434N1).
Keywords: Viral warts, Vitamin D3, Cryotherapy, Clinical trial
Copyright and License Information
© 2024 The Author(s).
This is an open access article distributed under the terms of the Creative Commons Attribution License (
http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Funding Statement
None.
Please cite this article as follows: Radmehr A, Ghareaghaji Zare A, Radmehr S, Abdossamadi Z. Therapeutic effects of intralesional injection of vitamin D3in treatment of recalcitrant warts: an evaluator-blinded clinical trial.Int J Drug Res Clin. 2024; 2: e10. doi: 10.34172/ijdrc.2024.e10
Introduction
Verruca vulgaris or viral warts are a prevalent infection worldwide caused by human papillomaviruses (HPV).1 Various treatment options are currently available for warts, which are determined depending on the patient’s condition, location, and number of warts; however, no particular and efficient antiviral medication and modality have been recognized for warts, and the current treatments often concentrate on destroying infected tissue.2 Some of these viruses have a strong carcinogenic potential and, if untreated, can lead to cancer.3 Physical deformity, pain, malfunction, psychological problems associated with warts, and the risk of transmission and cancer indicate that a wart needs to be treated. Destructive methods (e.g., cryotherapy, electrosurgery, surgery, and laser therapy), keratolytic drugs, immunotherapy, topical cytotoxic agents, and topical immunomodulators are commonly used as therapies.2,4
Cryotherapy is a widely used first treatment option for warts. This procedure involves exposing wart-infected tissue to cold temperatures to destroy it, but it often leads to adverse effects such as pain, blisters, scarring, and infection. In addition, patients must undergo therapy on multiple occasions to achieve the desired results. Vitamin D inhibits the proliferation of cells, triggers apoptosis and cell differentiation, regulates cytokines production, induces antibacterial peptides in the skin, and can be used as an immunotherapeutic agent when injected into lesions.5,6 The lower level of vitamin D in patients with viral warts suggested the association between the role of vitamin D and the treatment of viral warts.7
According to a study containing 64 patients with recalcitrant warts, the injection of 0.2- to 0.5-mL vitamin D3 solution led to a complete response in 90% of the patients. In this study, patients were followed up for 6 months to detect a possible recurrence, but only 3.33% of patients showed recurrence.8 In another study, in patients who suffered from plantar warts, after the injection of 0.2 mL of 7.5 mg/mL D3, 16 out of 20 patients experienced complete resolution of warts without major adverse effects.9 In a study conducted in 2020, vitamin D3 injection led to an appropriate improvement in the treatment of warts. A higher dosage was associated with a better response to treatment in this study, but the need for further evaluation was also mentioned in this study.10 The present study aimed to investigate the therapeutic effects of the intralesional injection of vitamin D in the treatment of recalcitrant warts which may accelerate the treatment process and reduce the burden imposed on patients.
Methods
Strategy and Patients
This clinical trial study was conducted in Sina hospital, Tabriz University of Medical Sciences (TUOMS) in which 40 patients were divided into two groups based on the patient’s attendance order at the dermatology clinic. In the first group, 20 participants received an intralesional injection of vitamin D3 combined with cryotherapy, and in the second group, 20 participants received just cryotherapy (Figure 1). The demographic characteristics of patients were collected, and if they matched our inclusion criteria, they were included in the trial. Some of these patients had undergone prior cryotherapy and topical cytotoxic and keratolytic medications before entering the trial, and we considered a 4-week washout period.
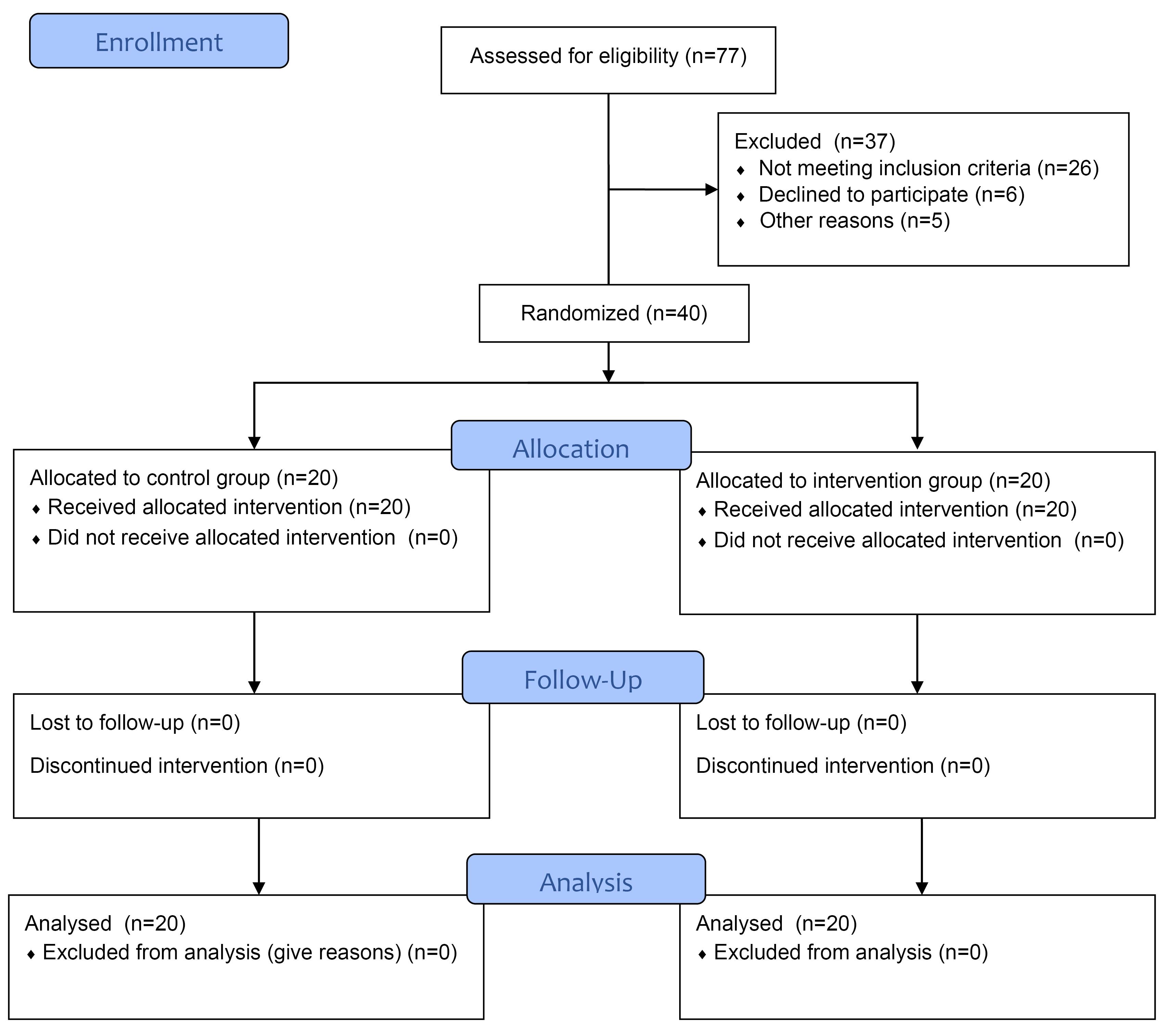
Figure 1.
Consort Flow Chart of the Study
.
Consort Flow Chart of the Study
In the 4 sessions of the treatment in each group, cryotherapy was conducted using cryospray from a 1 to 2-cm distance for 10-20 seconds. In the intervention group, this process was followed by an intradermal injection of 0.1 cc of vitamin D3 ampule (300 000 IU/1mL) per lesion and a maximum of 0.5 cc per session using a 27-gauge syringe. In each session, patients were evaluated for their response to treatment and complications by blinded evaluators. Finally, two groups were compared in terms of response to treatment and complications of the treatment, and patients were not monitored for recurrence after completing treatment sessions.
Having at least one recalcitrant wart (defined here as a wart that has not responded to usual treatment methods, including four sessions of cryotherapy or has remained stable for more than 6 months without receiving treatment) and informed consent were the inclusion criteria for this study. Exclusion criteria included warts on the face, mouth, or genital regions, pregnancy or breastfeeding, seizure, the inflammation of the injection site, cigarette smoking, chronic kidney disease, cold urticarial, hypervitaminoses D or hypercalcemia, and trypanophobia.
Furthermore, 100% recovery of the wart is defined as a complete response, improvement above 50% is defined as a moderate response, and less than 50% recovery is defined as a weak response to treatment.
Statistical Analysis
The statistical analysis was conducted by IBM SPSS v. 26 with 95% confidence intervals and a 0.05 level of significance. An independent sample t test was used for comparing the numerical variables, and the chi-square test was used for the non-numerical ones.
Results
Twenty patients were in the intervention group, and 20 patients were in the control group. The demographic characteristics of the patients involved in this study are mentioned in Table 1. The mean age of patients in the intervention group and the control group was 28.40 ± 10.96 and 24.85 ± 14.95 years, respectively. The intervention group consisted of 12 male and 8 female patients, while the control group consisted of 10 patients of each gender.
Table 1.
Demographic Characteristics of Patients (20 Patients in Each Group)
|
|
Intervention Group
(n=20)
|
Control Group
(n=20)
|
P
Value
|
| Age (y) (Mean ± SD) |
28.40 ± 10.96 |
24.85 ± 14.95 |
0.39 |
| Gender (female: male) |
8:12 |
10:10 |
0.52 |
| Duration (y) (Mean ± SD) |
2.16 ± 1.56 |
1.47 ± 1.04 |
0.11 |
| Previous treatments |
|
|
0.56 |
| None |
6 |
5 |
|
| Cryotherapy |
10 |
8 |
|
| Other modalities |
4 |
7 |
|
| Number of lesions |
1-4 |
1-4 |
0.59 |
Note. SD: Standard deviation.
Patients in the control group had a total of 45 lesions, and patients in the intervention group had a total of 45 lesions in hands, feet, palms and soles, forearms, legs, and thighs. Tables 2 and 3 illustrate the improvement of the wart after each session of injection. The rate of response following the completion of the treatment sessions was 95.33% in the vitamin D with cryotherapy group compared to 76.67% in the control group, and this difference is statistically significant (P < 0.01).
Table 2.
Improvement of Warts at Each Session of Treatment Based on the Mean Improvement Percent of All Warts in a Patient
|
Session
|
Group
|
Mean
|
SD
|
P
Value
|
| Session 1 |
Intervention |
46.00% |
21.12 |
< 0.01 |
| Control |
22.25% |
13.18 |
| Session 2 |
Intervention |
73.00% |
23.19 |
< 0.01 |
| Control |
39.00% |
20.74 |
| Session 3 |
Intervention |
84.50% |
16.37 |
0.04 |
| Control |
67.50% |
31.93 |
| Session 4 |
Intervention |
94.50% |
6.04 |
0.01 |
| Control |
77.00% |
27.54 |
Note. SD: Standard deviation.
Table 3.
Improvement of Warts at Each Session of Treatment Based on Improvement Percent of Each Lesion (45 Lesions in Each Group)
|
Session
|
Group
|
Mean
|
SD
|
P
Value
|
| Session 1 |
Intervention |
46.00% |
18.39 |
< 0.01 |
| Control |
24.22% |
12.62 |
| Session 2 |
Intervention |
70.67% |
20.60 |
< 0.01 |
| Control |
40.44% |
19.42 |
| Session 3 |
Intervention |
84.89% |
15.61 |
< 0.01 |
| Control |
64.44% |
26.51 |
| Session 4 |
Intervention |
95.33% |
5.88 |
< 0.01 |
| Control |
76.67% |
25.14 |
Note. SD: Standard deviation.
After completing the 4-session treatment, only 1 patient in the intervention group experienced a recovery rate of less than 90%, compared to 9 patients in the control group. In the intervention group, the minimum response rate was 80%, while it was only 30% in the control group.
Furthermore, 57.8% (26 out of 45) of the lesions in the intervention group were completely cured after 4 sessions (Figure 2), and the rest showed a moderate response to this treatment. In the control group, 37.7% (17 out of 45) of lesions completely recovered after completing the treatment process, 46.7% (21 out of 45) responded moderately to treatment, and 15.6% (7 out of 45) showed a weak response to treatment.
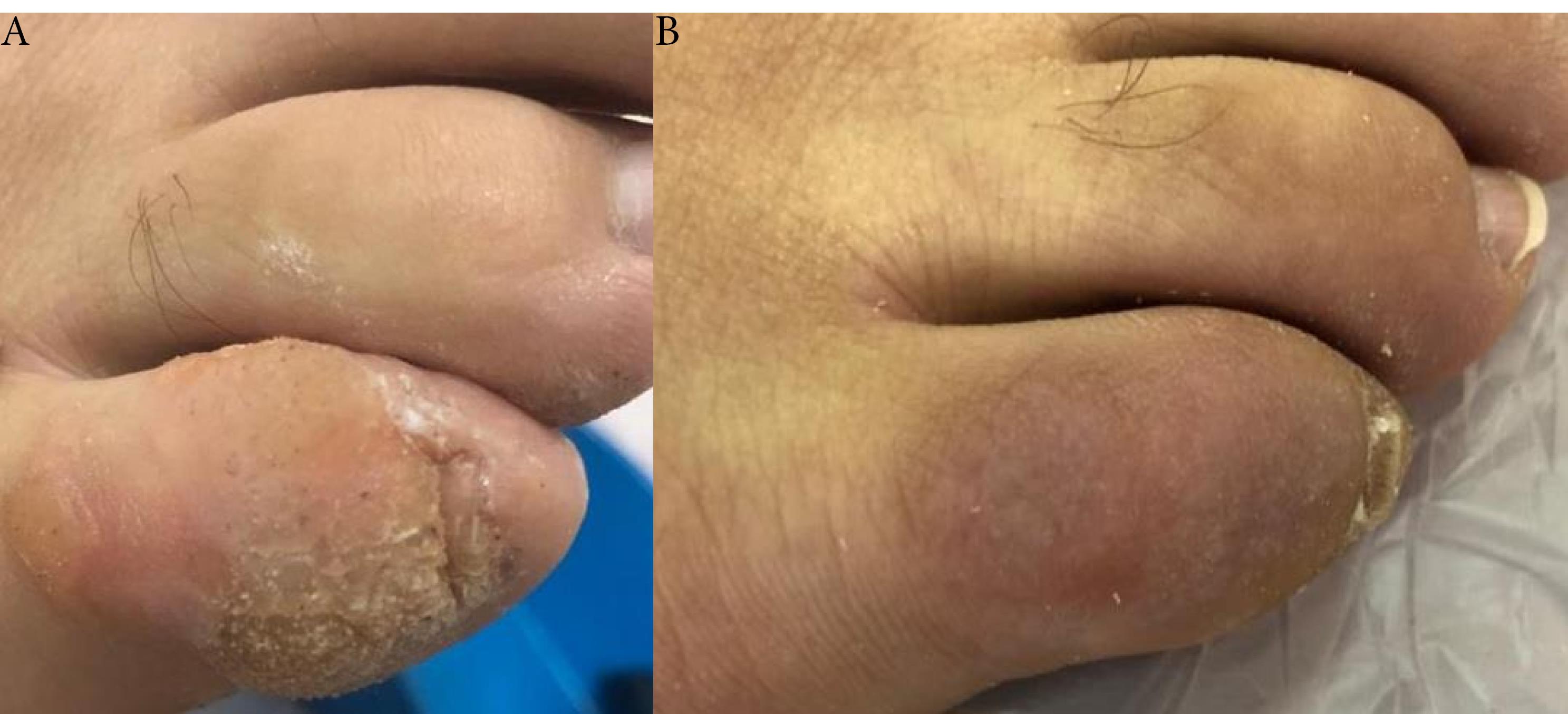
Figure 2.
Recalcitrant wart. A: before intervention (cryotherapy and intralesional injection of vitamin D) B: after 4 sessions of intervention (cryotherapy and intralesional injection of vitamin D)
.
Recalcitrant wart. A: before intervention (cryotherapy and intralesional injection of vitamin D) B: after 4 sessions of intervention (cryotherapy and intralesional injection of vitamin D)
The mean serum vitamin D in the intervention group patients was 22.75 ± 4.54 ng/mL before the start of the study and 40.95 ± 5.64 ng/mL after it, which was about an 18-unit increase in the systemic vitamin D in the patients in the intervention group, but none of the patients reached a hypervitaminosis D level. The serum vitamin D level in patients in the control group was not checked, but side effects of treatment were recorded during the treatment process, and patients in the intervention group experienced minimally increased pain as a result of the injection compared to those in the control group. In addition, blistering occurred in 4 patients in the control group and 3 patients in the intervention group. No other significant complications were observed during this study, and both interventions were well tolerated.
Discussion
This study aimed to compare the efficacy of intralesional injection of vitamin D3 alongside cryotherapy versus cryotherapy alone in the treatment of recalcitrant warts. After 4 treatment sessions, the healing rate of lesions in the group that received vitamin D was higher than that in the control group. Furthermore, 57% (26 out of 45) of the lesions in the intervention group were completely resolved after 4 sessions, and the rest showed a moderate response to this treatment. Except for mild to moderate pain during the injection, this treatment had no significant side effects for the patients.
Warts, in addition to their unpleasant appearance, can also develop into cancer.11 This procedure not only enhances the patient’s physical and psychological well-being, but it also has the potential to prevent skin cancer in the long run. According to a Turkish study on the correlation between vitamin D deficiency and skin lesions, HPV DNA survival rates were higher in vitamin D-deficient individuals than in non-deficient individuals. This difference is believed to be related to the anti-inflammatory role of vitamin D.12 However, the exact mechanism of vitamin D3’s action against warts is unclear. This can be accomplished by modifying immune system activation and cytokine production. Studies show that vitamin D is involved in regulating the immune system by inhibiting the expression of tumor necrosis factor-α and tumor necrosis factor-β, interleukin-6, and interleukin-8. It has also recently been demonstrated that the activation of toll-like receptors on human macrophages increases the expression of vitamin D receptor genes, which leads to the production of antimicrobial peptides.13 According to a study, intralesional triamcinolone (steroids were used as the first treatment option for keloids) and vitamin D are both statistically significantly effective in the management of keloids, and some complications such as atrophy and hypopigmentation in the vitamin D-receiving group were less than those in the other group. This study also found that the expression of vitamin D receptors in the patients of each group was not significantly different before and after treatment.14 Therefore, with further confirmation from other studies, vitamin D may be suggested as a therapy option.
Nasr et al investigated the therapeutic effects of intralesional injection of Candida antigen, vitamin D3, and combined digoxin and furosemide for the treatment of warts. According to their reports, complete response after 5 treatment sessions was 60% (15 out of 25 patients), 48% (12 out of 25), and 28% (7 out of 25), respectively. The response rate between the Candida antigen and vitamin D group was not statistically significant (P= 0.59), and they reported that intralesional Candida antigen and vitamin D were more effective than combined digoxin and furosemide. The recurrence rate after 6 months was 6.7% in Bleomycin, 25% in vitamin D, and 0% in combined digoxin and furosemide groups.15 Another study showed that the complete response rate after 4 treatment sessions at 2-week intervals in the intralesional Bleomycin group (22 patients) and the intralesional vitamin D group (26 patients) was 95.50% and 88.50%, respectively. Any recurrence after the 3-month follow-up was not reported.16
A different study compared the effectiveness of intralesional injection of vitamin D versus cryotherapy in plantar warts. The response to treatment was 63.4% and 43.4% (P = 0.21), respectively, and in specific age groups (41-50 years), the difference in treatment response between the two groups was significant.17 Aktaş et al observed that 80% of plantar warts completely responded to intralesional vitamin D injection without any recurrences after a 6-month follow-up. They injected 2 sessions of vitamin D at 1-month intervals.9 In the present study, after 4 sessions of treatment, the response rate in the intervention group was 95.33%, and it was 76.67% in the control group which shows a significant difference between the two modalities (P < 0.01).
According to a study in 2018, a higher rate of vitamin D deficiency was reported in patients with warts.7 Vitamin D3 injection is a low-cost intervention, and since it stimulates the immune system against HPV, the need for separate treatment of the lesions is likely to be eliminated.
The effects of other contributing factors should not be ignored. According to a study, the effects of aging and smoking were more significant than the effects of other clinical factors on the therapeutic efficacy of vitamin D injection.18 To eliminate these effects, we excluded smokers from our sample, and two groups were age-homogenized. Differences in response rates that are reported in studies can also be related to types and locations of warts, sample size, doses of injected agent, and the number of treatment sessions. To confirm the results of this study, it is necessary to design other studies with a larger sample size of patients and consider other contributing factors. Moreover, comparing the rate and speed of treatment response between cryotherapy with vitamin D injection and other immunotherapy modalities such as bleomycin injection and other injectable agents is one of the issues that can be considered by researchers. In addition, paraclinical investigations can help find the exact role of vitamin D in the treatment of skin warts.
Limitations
The limitation of this study was the small number of patients without a follow-up plan after completing the treatment sessions; furthermore, we did not evaluate spontaneous and distant wart resolutions. Moreover, we determined the study sample size based on the population that was accessible at the time the study was designed.
Conclusion
In conclusion, intralesional injection of vitamin D3 combined with cryotherapy for recalcitrant skin warts significantly increases the response to treatment without causing any particular complication. Further, this method reduces the number of patients’ visits to medical centers by accelerating the treatment process. In this way, it will reduce the financial burden imposed on patients, and the procedure will not cause serious side effects and scarring at the treatment site.
Ethics statement
The ethics committee of the Tabriz University of Medical Science approved this study (Ethics code: IR.TBZMED.REC.1398.1124).
Conflict of interests declaration
None.
Acknowledgments
None.
Data availability statement
The data supporting for this study’s findings are available on request from the corresponding author following the reasonable request.
Author contributions
Conceptualization: Afsaneh Radmehr, Zahra Abdossamadi.
Data curation: Zahra Abdossamadi, Armaghan Ghareaghaji Zare.
Formal analysis: Zahra Abdossamadi.
Funding acquisition: Afsaneh Radmehr.
Investigation: Armaghan Ghareaghaji Zare, Sina Radmehr.
Methodology: Afsaneh Radmehr andZahra Abdossamadi.
Project administration: Zahra Abdossamadi, Armaghan Ghareaghaji Zare.
Resources: Afsaneh Radmehr, Sina Radmehr.
Supervision: Armaghan Ghareaghaji Zare.
Validation: Afsaneh Radmehr.
Visualization: Afsaneh Radmehr, Sina Radmehr.
Writing–original draft: Zahra Abdossamadi.
Writing–review & editing: Sina Radmehr.
Consent for publication
Not applicable.
Trial Registration
This trial was registered in the Iranian Registry of Clinical Trials (IRCT code: IRCT20200513047434N1).
References
- Al Aboud AM, Nigam PK. Wart (plantar, verruca vulgaris, verrucae). In: StatPearls [Internet]. Treasure Island, FL: StatPearls Publishing; 2019.
- Ockenfels HM. Therapeutic management of cutaneous and genital warts. J Dtsch Dermatol Ges 2016; 14(9):892-9. doi: 10.1111/ddg.12838 [Crossref] [ Google Scholar]
- Piconese S, Cammarata I, Barnaba V. Viral hepatitis, inflammation, and cancer: a lesson for autoimmunity. J Autoimmun 2018; 95:58-68. doi: 10.1016/j.jaut.2018.10.021 [Crossref] [ Google Scholar]
- Moscarelli L, Annunziata F, Mjeshtri A, Paudice N, Tsalouchos A, Zanazzi M. Successful treatment of refractory wart with a topical activated vitamin D in a renal transplant recipient. Case Rep Transplant 2011; 2011:368623. doi: 10.1155/2011/368623 [Crossref] [ Google Scholar]
- Sassi F, Tamone C, D’Amelio P. Vitamin D: nutrient, hormone, and immunomodulator. Nutrients 2018; 10(11):1656. doi: 10.3390/nu10111656 [Crossref] [ Google Scholar]
- Samta Samta, Kumar S, Brar BK. Intralesional vitamin D3 for palmoplantar warts: a novel modality. J Pak Assoc Dermatol 2020; 30(3):418-22. [ Google Scholar]
- El Mongy NN, Hilal RF, Badr AM, Alraawi SA. Serum vitamin D level in patients with viral warts. J Egypt Womens Dermatol Soc 2018; 15(3):133-8. doi: 10.1097/01.EWX.0000544897.93500.a8 [Crossref] [ Google Scholar]
- Raghukumar S, Ravikumar BC, Vinay KN, Suresh MR, Aggarwal A, Yashovardhana DP. Intralesional vitamin D3 injection in the treatment of recalcitrant warts: a novel proposition. J Cutan Med Surg 2017; 21(4):320-4. doi: 10.1177/1203475417704180 [Crossref] [ Google Scholar]
- Aktaş H, Ergin C, Demir B, Ekiz Ö. Intralesional vitamin D injection may be an effective treatment option for warts. J Cutan Med Surg 2016; 20(2):118-22. doi: 10.1177/1203475415602841 [Crossref] [ Google Scholar]
- Chia-Han Yeh M, Tsai TY, Huang YC. Intralesional vitamin D3 injection in the treatment of warts: a systematic review and meta-analysis. J Am Acad Dermatol 2020; 82(4):1013-5. doi: 10.1016/j.jaad.2019.10.059 [Crossref] [ Google Scholar]
- Charny JW, Rady PL, Tyring SK, Kovarik CL. Malignant degeneration of diffuse intertriginous flat warts in a patient with AIDS. JAAD Case Rep 2018; 4(6):562-4. doi: 10.1016/j.jdcr.2018.02.006 [Crossref] [ Google Scholar]
- Özgü E, Yılmaz N, Başer E, Güngör T, Erkaya S, Yakut H. Could 25-OH vitamin D deficiency be a reason for HPV infection persistence in cervical premalignant lesions?. J Exp Ther Oncol 2016; 11(3):177-80. [ Google Scholar]
- AlGhamdi K, Kumar A, Moussa N. The role of vitamin D in melanogenesis with an emphasis on vitiligo. Indian J Dermatol Venereol Leprol 2013; 79(6):750-8. doi: 10.4103/0378-6323.120720 [Crossref] [ Google Scholar]
- Goyal A, Mehta H, Narang T, Vinay K, Dogra S. DS11 A double-blinded randomized control study to compare the effectiveness and safety of intralesional vitamin D3 with intralesional triamcinolone and its correlation with tissue expression of vitamin D receptors in patients with keloid. Br J Dermatol 2023; 188(Suppl 4):ljad113-250. doi: 10.1093/bjd/ljad113.250 [Crossref] [ Google Scholar]
- Nasr M, Abdelaty S, Elkholy BM. A comparative clinico-dermoscopic study of intralesional injection of combined digoxin and furosemide, Candida antigen, and vitamin D3 for multiple warts. J Cosmet Dermatol 2023; 22(4):1344-53. doi: 10.1111/jocd.15581 [Crossref] [ Google Scholar]
- Prathibha JP, Varghese N, Aithal VV. Intralesional vitamin D3 versus bleomycin for difficult-to-heal palmoplantar warts: a comparative study. J Cutan Aesthet Surg 2023; 16(2):114-20. doi: 10.4103/jcas.jcas_128_21 [Crossref] [ Google Scholar]
- Yousaf F, Raza N, Ahmed N, Sadiq S, Anwar A. Comparison of intralesional vitamin D3 versus cryotherapy for management of plantar warts. Pak Armed Forces Med J 2019; 69(6):1304-8. [ Google Scholar]
- El-Taweel AE, Salem RM, Allam AH. Cigarette smoking reduces the efficacy of intralesional vitamin D in the treatment of warts. Dermatol Ther 2019; 32(2):e12816. doi: 10.1111/dth.12816 [Crossref] [ Google Scholar]