Int J Drug Res Clin. 2023;1:e14.
doi: 10.34172/ijdrc.2023.e14
Review Article
The Advent of Artificial Intelligence in Anesthesiology and Pain Management: A Review Article
Kaveh Latifi 1  , Mohammad Negaresh 2 , Nima Javanshir 3 , Saeid Safari 4, *
, Mohammad Negaresh 2 , Nima Javanshir 3 , Saeid Safari 4, *
Author information:
1Department of Anesthesiology and Pain Medicine, School of Medicine, Iran University of Medical Sciences, Tehran, Iran
2Department of Internal Medicine, School of Medicine, Ardabil University of Medical Sciences, Ardabil, Iran
3School of Medicine, Ardabil University of Medical Sciences, Ardabil, Iran
4Functional Neurosurgery Research Center, Shohada Tajrish Comprehensive Neurosurgical Center of Excellence, Shahid Beheshti University of Medical Sciences, Tehran, Iran
Abstract
Background:
Artificial intelligence (AI) has brought about advancements in several areas, including anesthesiology. A description of the current state of the literature regarding the use of AI in relation to anesthesiology is needed to analyze whether AI is implemented in clinical anesthetic practice. AI and machine learning (ML) have been proven to be useful in developing effective healthcare strategies. Although AI has been employed to automate anesthetic delivery, it is not yet that common in anesthesiology and pain management.
Methods:
Various studies on the diverse uses of AI in the areas related to anesthesiology were compiled from several databases such as the Cochrane Library, Google Scholar, Medline (Ovid), and PubMed from 2003 to 2023. The obtained data were then classified, condensed, and juxtaposed finally. The study included diverse permutations of AI, ML, pain, and anesthesiology.
Results:
Postoperative pain has been one of the major concerns of anesthesiologists, and poor management in this regard can be associated with adverse events. In recent years, remarkable advances have been made in pain management strategies. One of them, which has attracted increasing attention, is the use of AI in anesthesiology and pain management. However, despite its great popularity, it has not been without challenges.
Conclusion:
In general, most of the studies explored in this review article have envisaged a bright future for the use of AI in anesthesiology and pain management. Some studies, however, have reported mixed results. Accordingly, further investigations with larger sample sizes are required to validate these findings.
Keywords: Artificial intelligence, Pain management, Anesthesiology
Introduction
Artificial intelligence (AI), also known as machine intelligence, refers to the general idea of creating machines that possess the ability to comprehend and execute tasks independently in an intelligent manner. Initial efforts towards automating medical processes were based on manually devised algorithms that relied on strict regulations, making them unsuitable for intricate clinical scenarios. Given the current scarcity of human resources in healthcare, utilizing technology to bridge the gaps seems to be a plausible solution.1 AI is characterized as the exploration of algorithms that empower machines to rationalize and execute such tasks as resolving issues, identifying objects, and making decisions.2 AI has been utilized in diverse areas of medicine, from diagnostic implementations in radiology3 and dementia diagnosis4 to more curative and interventional implementations in cardiology5 and surgery.6 Anesthesiology is a field that will likely benefit from advances in AI. Anesthesia can be subdivided into three main areas, including anesthesia, pain management, and intensive care medicine. There have been significant developments in this area of medicine, but the concept has essentially remained unchanged.7 Acomprehensive review was conducted regarding the impact of AI on anesthesia to identify AI techniques used in anesthesia and pain management. The alleviation of postoperative pain by administering analgesics is a major issue in perioperative medicine. The use of effective strategies aiming at enhancing recovery, optimizing pain management, and reducing the risk of pain-related complications should be of high priority.7-10 Therefore, better strategies should be developed to bridge the gap between the increasing demand for improved pain management and unsatisfactory practice in this regard.
Methods
Evidence Acquisition
This review explored studies conducted on the use of AI in anesthesia and pain management. A total of 43 articles were collected from various scientific databases, including Cochrane Library, Google Scholar, Embase, Medline Ovid, and PubMed. The selected articles were all related to AI and its role in pain management and had been published in the form of systematic reviews, evidence-based clinical practice guidelines, review articles, and randomized controlled trials. The applied keywords were AI, pain management, and anesthesia. A manual search was performed for references to ineligible articles in other studies that were not identified by a computerized search. Overall, 30 papers were identified at the end of this process. Finally, from among these articles, 15 papers that had the highest relevance to the topic were reviewed in detail (Figure 1).
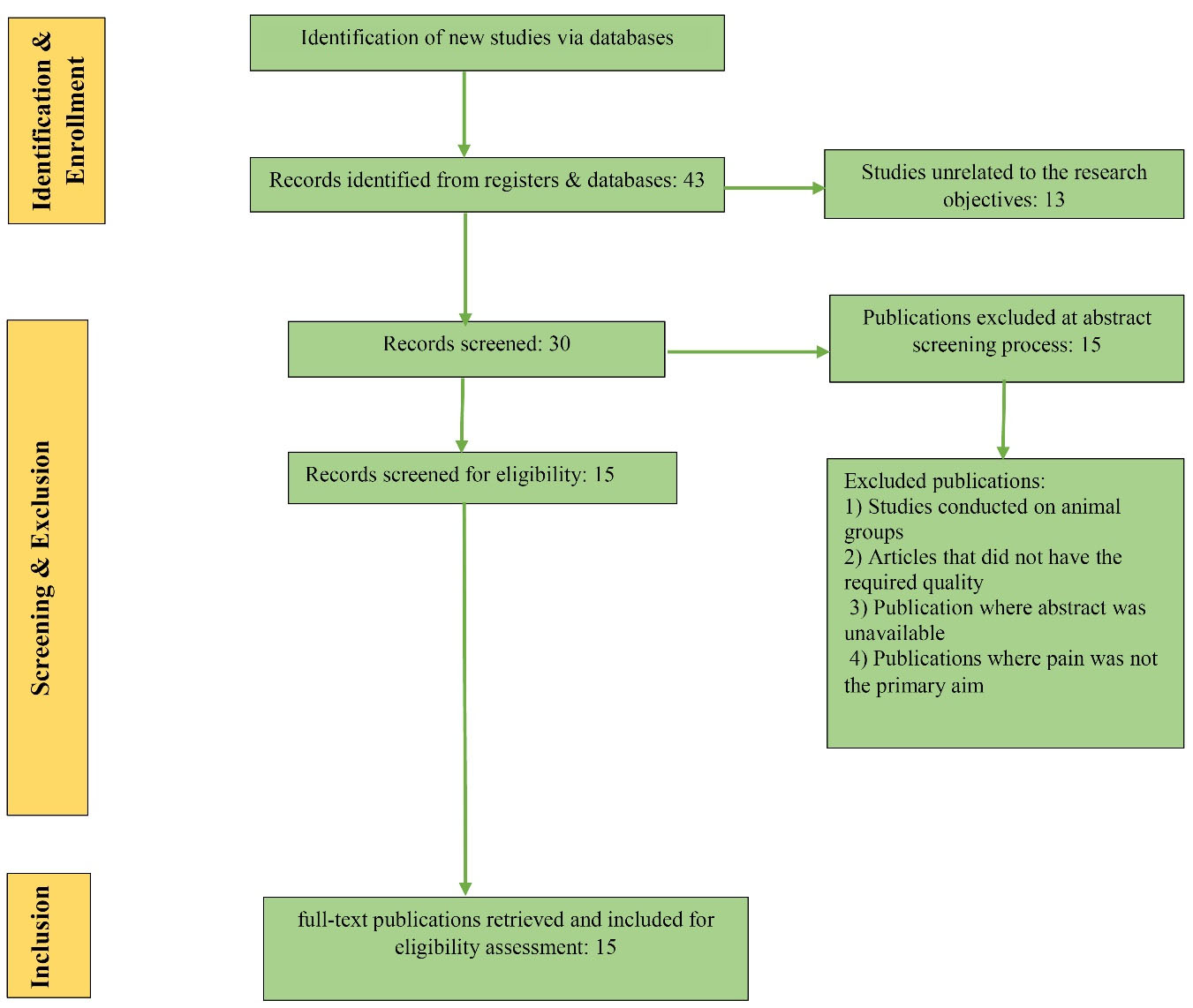
Figure 1.
Flowchart of the Study.
.
Flowchart of the Study.
Inclusion and Exclusion Criteria
Theinclusion criteria were using AI for pain management and investigating pain management in the field of anesthesiology. On the other hand, the exclusion criteria included publication without an abstract, lack of focus on pain as a primary variable, studies on animal groups, and lack of the required quality.
Results
The roots of AI probably date back to the 1940s, particularly 1942, when the American writer Isaac Asimov’s short story ‘Runaround’, a story about a robot invented by Gregory Powell and Mike, was published. Donavan has evolved with the three laws of robotics; A robot is not allowed to hurt a human being. In addition, a robot shall follow the instructions of human beings, except those that would not be compatible with the first law, and robots shall defend themselves as long as such protection does not conflict with the first or second laws.11 In recent years, there has been a great deal of interest among researchers in the role of AI in various fields of medicine. One such area is pain management, in which partial successes have been achieved, but they need to be expanded.12 Pain is a physiologic response to a noxious stimulus. Severe untreated perioperative pain affects not only the respiratory, circulatory, and immune systems, but the patient’s convalescence as well.13 Postoperative pain management has always been a serious concern for anesthesiologists. In recent years, significant progress has been made in various surgical procedures, from the use of intravenous opioid or non-opioid drugs14 to the use of ultrasound-guided methods.15
Pain Alleviation Before and After the Advent of AI
Clinicians believe that clinical practice guidelines may lead to better health outcomes. Guidelines provide useful information that can be used by physicians in making decisions about patient care. The federal government, through the Agency for Health Policy and Research, began to facilitate the development of clinical practice guidelines in 1992.16 Several national studies have been conducted regarding postoperative pain management. A US national survey of 300 adults who underwent surgery demonstrated that nearly 86% of the cases experienced pain after surgery. Of these cases, 75% experienced moderate to severe pain immediately after surgery, and 74% continued to experience similar pain after discharge. Approximately 88% of the cases received analgesics to reduce pain. Of these, 80% experienced side effects, and 39% reported moderate to severe pain after the first dose.17 In another study, a systemic review and meta-analysis was performed on 765 patients with chronic postoperative pain, of whom 38.82% had previously experienced acute postoperative pain. The risk ratio of chronic postoperative pain in patients with acute postoperative pain, as compared to those without it, was 3.10 (95% confidence interval: 2.44, 3.96).18 A national survey was conducted on postoperative pain management in a sample of 76 surgical centers in France from June 2004 to July 2006. Data were collected from 1900 adult patients. The reported postoperative pain was mild at rest [2.7 (1.3)], moderate during exercise [4.9 (1.9)], and strong at peak [6.4 (2.0)].19 In a study conducted in 2008, the incidence of postoperative pain in a sample of 1490 patients underwent investigation. The results were disappointing; moderate to severe pain was reported in 41% of the patients on day 0, 30% on day 1, and 19%, 16%, and 14% on days 2, 3, and 4, respectively. The frequency of moderate to severe pain on days 1-4 was high in the limb surgery (20%-71%) and spine surgery (30%-64%) groups.20 AI-enabled technologies and algorithms are on the rise and are currently transforming the healthcare landscape. AI has overtaken humans in several medical fields such as diagnosing diseases based on medical and pathological imaging or monitoring disease activity in atrial fibrillation and epilepsy relapses.21-23 AI has six main clinical applications in anesthesiology, including depth of anesthesia monitoring, control of anesthesia, event and risk prediction, ultrasound guidance, pain management, and operating room logistics.24 A study examined whether AI could be used as a decision support tool to improve anesthesiologists’ predictions of postoperative opioid needs.25 They were asked to predict postoperative opioid requirements for 100 surgical patients with and without using ML model estimates of opioid requirements. The accuracy of anesthesiologist’s estimates with and without ML estimates as the reference was compared, and the accuracy of opioid requirement estimation increased from 18% without ML support to 42% (P < 0.001) when ML estimates were provided as the reference. They concluded that ML models could improve the assessments of clinical parameters by anesthesiologists, and ML predictions could primarily serve as a reference to correct anesthesiologists’ clinical assessments. In 2021, another systematic review was conducted to examine the clinical use of ML in the diagnosis, classification, and management of pain. To this end, 26 research articles related to pain and ML were investigated, and most of the included studies used ML algorithms to effectively classify the patients’ pain levels and predict pain development and management. Based on the results obtained in this review, several studies indicated that the use of ML in pain research was of great importance as it was proved to be highly useful in the classification, prediction, diagnosis, and treatment of pain.26 Another study was performed on anesthesiologists’ attitudes toward the utilization of AI in anesthesia practices in developing countries. Based on the results, although the majority of anesthesiologists (88.6%) had heard of AI, only 6.8% believed they knew enough about it. Of them, 68.2% declared that AI had useful applications in anesthesia practice, and 56.8% believed that AI would bring breathtaking changes to their field. Few respondents (13.6%) believed that AI would surpass the clinical capabilities of human anesthesiologists and would completely replace human anesthesiologists in the future (6.8%). There was a significant association between clinical practice and the belief that AI could be effectively used in anesthesia practice. Moreover, a significant association was observed between the perception of AI and the belief that its capabilities were currently superior to the clinical experience of human anesthesiologists.27 Another study assessed the future of AI and anesthesiology aiming at investigating whether anesthesiologists’ opinions, motivations, and perceived barriers to using AI in clinical settings are associated with physician-level and real-world characteristics. Invitations to the study were emailed to 27 056 anesthesiologists working in the US. From May 2021 to June 2021, 1086 physicians (4%) responded to the survey. When predicting the future role of AI in this field, anesthesiologists believed that AI could help predict perioperative adverse events (83%), develop pain management plans (67%), and perform airway assessments (45%). The majority of the respondents did not believe that AI would surpass human beings in providing healthcare services for patients (81%), performing endotracheal intubation (65%), and performing local anesthesia blocks (64%). The top barriers to using AI in clinical practice were found to be a lack of algorithmic transparency (60%), malpractice and liability concerns (47%), and the potential for malpractice (41%).28
Discussion
Artificial intelligence and its subsets utilize information and algorithms to replicate the process of human cognition and education. Machine learning (ML) is a branch of AI that helps you make AI-based operations. Deep learning itself is a branch of ML that uses a vast pool of data and algorithms to train a model. To gradually inform and improve the accuracy of algorithms, ML employs a set of methods for automatically detecting patterns in large data. These patterns are applied for the classification, prediction, or extraction of information from forthcoming data to which an algorithm has been able to infer new knowledge. Specifically, algorithm training is conducted to develop classifications or predictions based on statistical techniques that reveal key findings from data mining projects. Different techniques are applied for managing ML in line with the nature of the data.26 Most of the studies included in this review have been published from 2015 on, suggesting an increase in the use of AI for pain management issues in recent years. The main finding of this study is that using AI in the pain branch of anesthesiology, which is rapidly expanding, can yield positive outcomes. The results of the application of AI and ML in medical fields have been promising. Since its first use to automate the administration of anesthetics, AI has made many strides in its introduction into the field of anesthesiology, but it is still uncommon. The existing literature has indicated that ML calculations are of great value in pain management. Although such tools can ultimately support anesthesiologists’ clinical decision-making, it is still unclear how real-time ML-based predictions will be governed. The area of postoperative pain management has benefited from AI by developing software programs that can predict pain levels and analgesic requirements, which, in turn, has made personalized care increasingly achievable. Furthermore, ML techniques not only aid in the provision of direct patient care but also provide highly accurate clinical scenarios and strict feedback that enhance simulation training capabilities, thereby potentially improving anesthesiology education.AI has extensive applications in anesthesia care as it provides real-time information about patients and allows doctors to focus on more complex tasks. However, more investigations are needed to fully understand what role AI will play in anesthesiology.29 As hinted above, AI is defined as “the study of algorithms that give machines this capability to deduce and perform tasks such as problem-solving, reasoning, and decision-making.”30 The articles reviewed in the current investigation represent that AI is believed to be extremely helpful in classifying, predicting, diagnosing, and managing pain. However, ambiguity remains in some related aspects. Although algorithms can be used to train machines to perform specific input-output mappings, it is often unclear which parts of the training network are responsible for specific results. This is undesirable, as the physician must understand and trust how the autonomic anesthesia system works.7 Anesthesiologists should continue to use this technology, stay abreast of the advances in AI, and make a real effort to seamlessly integrate it into their daily practice so that they can become their future revolutionaries. We hope to witness more widespread use of AI in all areas of medical practice, and anesthesiology is no exception. It is time for our colleagues to start visualizing various uses of AI in practice.30 In summary, the literature highlights the lack of knowledge about AI in anesthesiology and the acceptance of its use in practice among anesthesiologists. Although AI is believed to be useful in anesthesia practice and offers a wide range of applications and benefits, it is not expected to surpass or replace human anesthesiologists. There are also concerns about AI’s ability to provide empathetic, patient-focused care and its effectiveness in unforeseen circumstances. Overall, clinical care anesthesiologists have better judgments than AI.28 We recommend that further studies should be conducted on more anesthesiologists to better determine their quantitative knowledge regarding AI and gain a deeper and broader understanding of their attitudes towards the use of AI in clinical practice.
Conclusion
Overall, most of the reviewed studies envisage a bright future for the application of AI in anesthesiology and pain management. Some studies, however, yielded mixed results, suggesting that further investigations with larger sample sizes are necessary to validate these findings.
Ethics statement
Not applicable.
Disclosure of funding source
None.
Conflict of interests declaration
There is nothing to declare.
Acknowledgments
None.
Data availability statement
Supporting data for this study are available and will be provided to the applicant upon reasonable request from the corresponding author.
Consent for publication
Not applicable.
References
- Singh M, Nath G. Artificial intelligence and anesthesia: a narrative review. Saudi J Anaesth 2022; 16(1):86-93. doi: 10.4103/sja.sja_669_21 [Crossref] [ Google Scholar]
- Mintz Y, Brodie R. Introduction to artificial intelligence in medicine. Minim Invasive Ther Allied Technol 2019; 28(2):73-81. doi: 10.1080/13645706.2019.1575882 [Crossref] [ Google Scholar]
- Thrall JH, Li X, Li Q, Cruz C, Do S, Dreyer K. Artificial intelligence and machine learning in radiology: opportunities, challenges, pitfalls, and criteria for success. J Am Coll Radiol 2018; 15(3 Pt B):504-8. doi: 10.1016/j.jacr.2017.12.026 [Crossref] [ Google Scholar]
- Zarei M, Asheghi M, Zarei M. Artificial intelligence in dementia diagnosis: past, present, and future. Int J Aging 2023; 1(1):e14. doi: 10.34172/ija.2023.e14 [Crossref] [ Google Scholar]
- Deo RC. Machine learning in medicine. Circulation 2015; 132(20):1920-30. doi: 10.1161/circulationaha.115.001593 [Crossref] [ Google Scholar]
- Hashimoto DA, Rosman G, Rus D, Meireles OR. Artificial intelligence in surgery: promises and perils. Ann Surg 2018; 268(1):70-6. doi: 10.1097/sla.0000000000002693 [Crossref] [ Google Scholar]
- McGrath H, Flanagan C, Zeng L, Lei Y. Future of artificial intelligence in anesthetics and pain management. J Biosci Med 2019; 7(11):111-8. doi: 10.4236/jbm.2019.711010 [Crossref] [ Google Scholar]
- Gerbershagen HJ, Pogatzki-Zahn E, Aduckathil S, Peelen LM, Kappen TH, van Wijck AJ. Procedure-specific risk factor analysis for the development of severe postoperative pain. Anesthesiology 2014; 120(5):1237-45. doi: 10.1097/aln.0000000000000108 [Crossref] [ Google Scholar]
- Gerbershagen HJ, Rothaug J, Kalkman CJ, Meissner W. Determination of moderate-to-severe postoperative pain on the numeric rating scale: a cut-off point analysis applying four different methods. Br J Anaesth 2011; 107(4):619-26. doi: 10.1093/bja/aer195 [Crossref] [ Google Scholar]
- Schwenkglenks M, Gerbershagen HJ, Taylor RS, Pogatzki-Zahn E, Komann M, Rothaug J. Correlates of satisfaction with pain treatment in the acute postoperative period: results from the international PAIN OUT registry. Pain 2014; 155(7):1401-11. doi: 10.1016/j.pain.2014.04.021 [Crossref] [ Google Scholar]
- Haenlein M, Kaplan A. A brief history of artificial intelligence: on the past, present, and future of artificial intelligence. Calif Manage Rev 2019; 61(4):5-14. doi: 10.1177/0008125619864925 [Crossref] [ Google Scholar]
- Gupta B, Sahay N, Vinod K, Sandhu K, Basireddy HR, Mudiganti RKR. Recent advances in system management, decision support systems, artificial intelligence and computing in anaesthesia. Indian J Anaesth 2023; 67(1):146-51. doi: 10.4103/ija.ija_974_22 [Crossref] [ Google Scholar]
- Brennan F, Cousins MJ. Pain relief as a human right. Pain Clin Updates 2004; 12(5):1-4. [ Google Scholar]
- Schug SA, Garrett WR, Gillespie G. Opioid and non-opioid analgesics. Best Pract Res Clin Anaesthesiol 2003; 17(1):91-110. doi: 10.1053/bean.2003.0267 [Crossref] [ Google Scholar]
- Rahimzadeh P, Faiz SHR, Latifi-Naibin K, Alimian M. A Comparison of effect of preemptive versus postoperative use of ultrasound-guided bilateral transversus abdominis plane (TAP) block on pain relief after laparoscopic cholecystectomy. Sci Rep 2022; 12(1):623. doi: 10.1038/s41598-021-04552-6 [Crossref] [ Google Scholar]
- McCormick KA, Fleming B. Clinical practice guidelines The Agency for Health Care Policy and Research fosters the development of evidence-based guidelines. Health Prog 1992; 73(10):30-4. [ Google Scholar]
- Mei WJ, Fei LH, Yan JH. Acute post surgical pain may result in chronic post surgical pain: a systemic review and meta analysis. Pak J Med Sci 2015; 31(4):833-6. doi: 10.12669/pjms.314.7555 [Crossref] [ Google Scholar]
- Telci L, Esen F, Akcora D, Erden T, Canbolat T, Akpir K. Evaluation of effects of magnesium sulphate in reducing intraoperative anaesthetic requirements. BJA: British Journal of Anaesthesia 2002; 89(4):594-598. doi: 10.1093/bja/aef238 [Crossref] [ Google Scholar]
- Fletcher D, Fermanian C, Mardaye A, Aegerter P. A patient-based national survey on postoperative pain management in France reveals significant achievements and persistent challenges. Pain 2008; 137(2):441-51. doi: 10.1016/j.pain.2008.02.026 [Crossref] [ Google Scholar]
- Sommer M, de Rijke JM, van Kleef M, Kessels AG, Peters ML, Geurts JW. The prevalence of postoperative pain in a sample of 1490 surgical inpatients. Eur J Anaesthesiol 2008; 25(4):267-74. doi: 10.1017/s0265021507003031 [Crossref] [ Google Scholar]
- Attia ZI, Noseworthy PA, Lopez-Jimenez F, Asirvatham SJ, Deshmukh AJ, Gersh BJ. An artificial intelligence-enabled ECG algorithm for the identification of patients with atrial fibrillation during sinus rhythm: a retrospective analysis of outcome prediction. Lancet 2019; 394(10201):861-7. doi: 10.1016/s0140-6736(19)31721-0 [Crossref] [ Google Scholar]
- Kearney H, Byrne S, Cavalleri GL, Delanty N. Tackling epilepsy with high-definition precision medicine: a review. JAMA Neurol 2019; 76(9):1109-16. doi: 10.1001/jamaneurol.2019.2384 [Crossref] [ Google Scholar]
- Briganti G, Le Moine O. Artificial intelligence in medicine: today and tomorrow. Front Med (Lausanne) 2020; 7:27. doi: 10.3389/fmed.2020.00027 [Crossref] [ Google Scholar]
- Hashimoto DA, Witkowski E, Gao L, Meireles O, Rosman G. Artificial intelligence in anesthesiology: current techniques, clinical applications, and limitations. Anesthesiology 2020; 132(2):379-94. doi: 10.1097/aln.0000000000002960 [Crossref] [ Google Scholar]
- Velagapudi M, Nair AA, Strodtbeck W, Flynn DN, Howell K, Liberman JS. Evaluation of machine learning models as decision aids for anesthesiologists. J Clin Monit Comput 2023; 37(1):155-63. doi: 10.1007/s10877-022-00872-8 [Crossref] [ Google Scholar]
- Matsangidou M, Liampas A, Pittara M, Pattichi CS, Zis P. Machine learning in pain medicine: an up-to-date systematic review. Pain Ther 2021; 10(2):1067-84. doi: 10.1007/s40122-021-00324-2 [Crossref] [ Google Scholar]
- Ejikem M, Eya J, Ibu F. Perspectives of anesthesiologists towards the use of artificial intelligence in anesthesia practice in a developing country. J Anaesth Surg Res 2022; 3(1):1-10. doi: 10.37191/Mapsci-JASR-3(1)-019 [Crossref] [ Google Scholar]
- Alamo CE, Lane-Fall M. Artificial intelligence and the future of anesthesiology: qualitative findings from a national survey of physician anesthesiologists. Anesth Analg 2022; 134(4 Suppl):46. [ Google Scholar]
- Cote CD, Kim PJ. Artificial intelligence in anesthesiology: moving into the future. Univ Toronto Med J 2019; 96(1):33-5. [ Google Scholar]
- Bellman R. An Introduction to Artificial Intelligence: Can Computer Think? Thomson Course Technology; 1978.